The Impact of Antenatal Corticosteroids on Late Preterm Twin Deliveries: A Critical Review
2025-03-19
Author: Daniel
Introduction
Preterm birth remains a leading cause of complications and fatalities in newborns worldwide, defined as any live birth that occurs before 37 weeks of gestation. The challenges are particularly pronounced in twin pregnancies, where a staggering 61.27% of multifetal pregnancies result in preterm births, according to a 2022 report from the National Vital Statistics in the United States.
Classification of Preterm Births
The World Health Organization categorizes preterm births into three segments: moderate to late preterm (32–37 weeks), very preterm (28–32 weeks), and extreme preterm (<28 weeks). In twin pregnancies, late preterm births (between 34 0/7 and 36 6/7 weeks) account for over 60% of live births.
Current Research Focus
Research primarily concentrates on infants born before 34 weeks due to their heightened risk of severe complications. Antenatal corticosteroid treatment (ACT) aims to enhance fetal lung maturity and is routinely offered to women at risk of preterm delivery before reaching 34 weeks. However, the effectiveness of ACT for late preterm infants remains uncertain, with studies presenting mixed results regarding its impact on neonatal complications.
Risks for Late Preterm Infants
Despite late preterm infants exhibiting lower neonatal complications than those born earlier, they still face risks higher than term infants. A significant gap in understanding persists around the administration of ACT in twin pregnancies delivering after 34 weeks, prompting the need for in-depth research.
Recent Study Overview
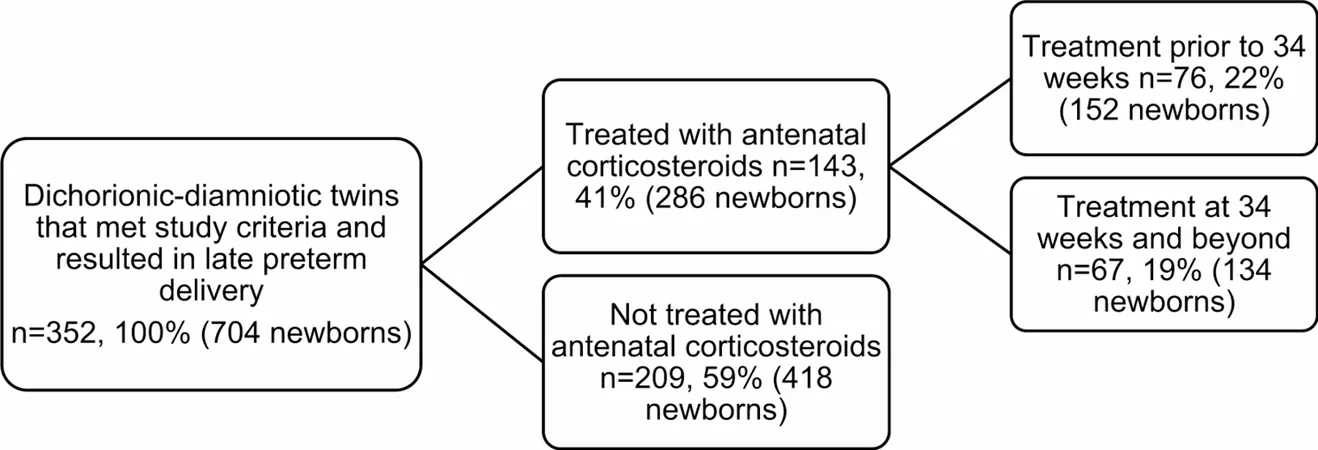
In a recent retrospective cohort study, researchers evaluated neonatal outcomes in dichorionic-diamniotic twin pregnancies delivered late preterm, contrasting those who received ACT with those who did not. The study reviewed medical records from over 69,000 births between 2017 and 2021 at a leading medical center in Turkey, focusing on pregnancies that remained stable at the time of admission but later required intervention.
Findings of the Study
The study culminated with 352 eligible women, segments of whom received ACT at varying gestational ages. Findings indicated crucial distinctions in neonatal outcomes based on the timing of ACT administration. Notably, rates of neonatal hypoglycemia surged among infants exposed to treatment before 34 weeks compared to unexposed counterparts.
Beyond hypoglycemia, the research corroborated earlier findings suggesting higher rates of neonatal intensive care unit (NICU) admissions among those receiving ACT, regardless of timing. Additionally, the study revealed that greater gestational age and higher birthweight significantly correlate with improved neonatal outcomes.
Implications for Clinical Practice
These revelations underline the pressing need to refine guidelines surrounding ACT application in multiple pregnancies, particularly in the late preterm timeframe. Current practice, largely informed by data from singleton pregnancies, may not aptly reflect the unique circumstances of twin gestation.
As twin pregnancies often encounter specialized challenges, including shared resources and space, it becomes imperative to investigate tailored corticosteroid protocols that address these specific dynamics.
Conclusion
In conclusion, while ACT carries benefits for preterm deliveries, caution is warranted, especially regarding its administration in twin pregnancies. As we advance, further investigations are essential to glean a comprehensive understanding of ACT's risk-benefit profile, potentially reshaping clinical strategies for managing high-risk twin pregnancies. The future may hold more refined approaches to enhance twins’ wellbeing without compromising their health during critical developmental stages.




 Brasil (PT)
Brasil (PT)
 Canada (EN)
Canada (EN)
 Chile (ES)
Chile (ES)
 Česko (CS)
Česko (CS)
 대한민국 (KO)
대한민국 (KO)
 España (ES)
España (ES)
 France (FR)
France (FR)
 Hong Kong (EN)
Hong Kong (EN)
 Italia (IT)
Italia (IT)
 日本 (JA)
日本 (JA)
 Magyarország (HU)
Magyarország (HU)
 Norge (NO)
Norge (NO)
 Polska (PL)
Polska (PL)
 Schweiz (DE)
Schweiz (DE)
 Singapore (EN)
Singapore (EN)
 Sverige (SV)
Sverige (SV)
 Suomi (FI)
Suomi (FI)
 Türkiye (TR)
Türkiye (TR)
 الإمارات العربية المتحدة (AR)
الإمارات العربية المتحدة (AR)